Therapeutic/Pharmacologic Class of Drug: Tocilizumab is a recombinant humanized anti-human interleukin-6 (IL-6) receptor monoclonal antibody of the immunoglobulin (Ig) IgG
1 subclass.
ATC Code: L04AC07.
Pharmacology: Pharmacodynamics: In clinical studies with tocilizumab in RA, rapid decreases in C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), serum amyloid A and fibrinogen were observed. Increases in haemoglobin levels were observed, through tocilizumab decreasing the IL-6 driven effects on hepcidin production to increase iron availability.
In study WA28119, similar rapid decreases in CRP and ESR were observed along with slight increases in mean corpuscular haemoglobin concentration.
In healthy subjects administered tocilizumab in doses from 2 to 28 mg/kg, absolute neutrophil counts decreased to their lowest 3 to 5 days following administration. Thereafter, neutrophils recovered towards baseline in a dose dependent manner. Rheumatoid arthritis and GCA patients demonstrated a similar pattern of absolute neutrophil counts following tocilizumab administration (see General under Precautions).
Mechanism of Action: Tocilizumab is a recombinant humanized anti-human interleukin-6 (IL-6) receptor monoclonal antibody of the immunoglobulin (Ig) IgG
1 subclass. Tocilizumab binds to both soluble and membrane-bound IL-6 receptors (sIL-6R and mIL-6R), and has been shown to inhibit sIL-6R and mIL-6R-mediated signaling. IL-6 is a multi-functional cytokine, produced by a variety of cell types involved in local paracrine function as well as regulation of systemic physiological and pathological processes such as induction of immunoglobulin secretion, T-cell activation, induction of hepatic acute phase proteins and stimulation of haematopoiesis. IL-6 has been implicated in the pathogenesis of diseases including inflammatory diseases, osteoporosis, and neoplasia.
The possibility exists for tocilizumab to affect host defences against infections and malignancies. The role of Il-6 receptor inhibition in the development of malignancies is not known.
Clinical/Efficacy Studies: Rheumatoid Arthritis: The efficacy of intravenously administered tocilizumab in alleviating the signs and symptoms of rheumatoid arthritis was assessed in five randomized, double-blind, multicentre studies. Studies I-V required patients ≥ age 18 with active rheumatoid arthritis diagnosed according to American College of Rheumatology (ACR) criteria who had at least 8 tender and 6 swollen joints at baseline.
Tocilizumab was administered intravenously every 4 weeks as monotherapy (Study I), in combination with MTX (Studies II, III, V) or with other disease-modifying anti-rheumatic drugs (DMARDs) (Study IV).
Study I evaluated 673 patients who had not been treated with MTX within 6 months prior to randomization, and who had not discontinued previous MTX treatment as a result of clinically important toxic effects or lack of response. The majority (67%) of patients were MTX naïve. Doses of 8 mg/kg of tocilizumab were given every four weeks as monotherapy. The comparator group was weekly MTX (dose titrated from 7.5 to a maximum of 20 mg weekly over an 8 week period). The primary endpoint was the proportion of patients who achieved an ACR20 response at week 24.
Study II, a 2 year study, evaluated 1196 patients who had an inadequate clinical response to MTX. Doses of 4 or 8 mg/kg of tocilizumab or placebo were given every four weeks as blinded therapy for 52 weeks, in combination with stable MTX (10 - 25 mg weekly). The primary endpoint at week 24 was the proportion of patients who achieved ACR20 response criteria. At week 52 the co-primary endpoints were prevention of joint damage and improvement in physical function.
Study III evaluated 623 patients who had an inadequate clinical response to MTX. Doses of 4 or 8 mg/kg of tocilizumab or placebo were given every four weeks, in combination with stable MTX (10 - 25 mg weekly). Study IV evaluated 1220 patients who had an inadequate response to their existing rheumatologic therapy, including one or more DMARDs. Doses of 8 mg/kg tocilizumab or placebo were given every four weeks, in combination with the stable DMARD. Study V evaluated 499 patients who had an inadequate clinical response or were intolerant to one or more anti-TNF therapies. The anti-TNF agent was discontinued prior to randomization. Doses of 4 or 8 mg/kg of tocilizumab or placebo were given every four weeks, in combination with stable MTX (10 - 25 mg weekly). The primary endpoint for studies III-V was the proportion of patients who achieved an ACR20 response at week 24.
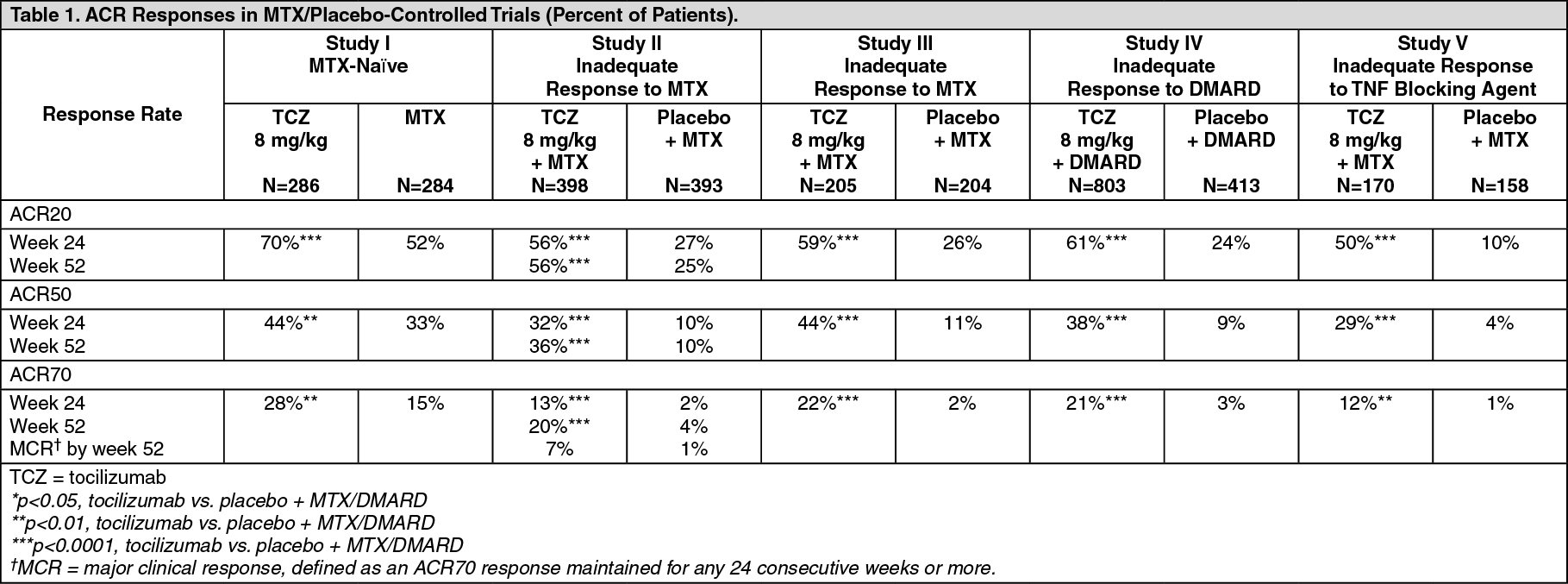
The percent of patients achieving ACR 20, 50 and 70 responses in Studies I to V are shown in Table 1.
The efficacy of subcutaneously administered tocilizumab was assessed in a double-blind, controlled, multicentre study in patients with active RA. The study (SC-I) required patients to be above 18 years of age with active rheumatoid arthritis diagnosed according to ACR criteria and who had at least 4 tender and 4 swollen joints at baseline. All patients received background non-biologic DMARD(s).
Study SC-I evaluated patients with moderate to severe active rheumatoid arthritis who had an inadequate clinical response to their existing rheumatologic therapy, including one or more DMARD(s). Approximately 20% had a history of inadequate response to at least one TNF inhibitor. In SC-I, 1262 patients were randomized 1:1 to receive tocilizumab SC 162 mg every week or tocilizumab IV 8 mg/kg every four weeks in combination with non-biologic DMARD(s). The primary endpoint in the study was the difference in the proportion of patients who achieved an ACR20 response at week 24. The results from study SC-I is shown in Table 3. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In all studies, 8 mg/kg tocilizumab-treated patients had statistically significant higher ACR20, 50, 70 response rates at 6 months compared to control. The treatment effect was similar in patients independent of rheumatoid factor status, age, gender, race, number of prior treatments or disease status. Time to onset was rapid (as early as week 2) and the magnitude of response continued to improve with duration of treatment. Continued durable responses were seen for over 3 years in the open label extension studies of Studies I-V.
In the 8 mg/kg tocilizumab-treated patients significant improvements were noted on all individual components of the ACR response (tender and swollen joint counts, patient and physician global assessment, disability index scores (HAQ), pain assessment and CRP compared to patients receiving placebo+MTX/DMARDS in all studies.
Tocilizumab 8 mg/kg treated patients had a statistically significantly greater reduction in disease activity score (DAS28) than patients treated with placebo+DMARD. A good to moderate EULAR response was achieved by significantly more tocilizumab treated patients compared to patients treated with placebo+DMARD (Table 2). (See Tables 2 and 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Major Clinical Response: After 2 years of treatment with tocilizumab/MTX, 14% of patients achieved a major clinical response (maintenance of an ACR70 response for 24 weeks or more).
Radiographic Response – Intravenous Administration: In Study II, in patients with an inadequate response to MTX, inhibition of structural joint damage was assessed radiographically and expressed as change in modified Sharp score and its components, the erosion score and joint space narrowing score. Inhibition of joint structural damage was shown with significantly less radiographic progression in patients receiving tocilizumab compared to control.
In the open-label extension of Study II the inhibition of progression of structural damage in tocilizumab/MTX-treated patients was maintained in the second year of treatment. (See Table 4.)
Click on icon to see table/diagram/image
Following 1 year of treatment with tocilizumab/MTX, 83% of patients had no progression of structural damage, as defined by a change in the TSS score of zero or less, compared with 67% of placebo/MTX-treated patients. This remained consistent following 2 years of treatment (83%). Ninety three percent (93%) of patients had no progression between week 52 and week 104.
Radiographic Response – Subcutaneous Administration: The radiographic response of subcutaneously administered tocilizumab was assessed in a double-blind, controlled, multicentre study in patients with active RA. This study (SC-II) evaluated patients with moderate to severe active rheumatoid arthritis who had an inadequate clinical response to their existing rheumatologic therapy, including one or more DMARD(s) where approximately 20% had a history of inadequate response to at least one TNF inhibitor. Patients were required to be above 18 years of age with active rheumatoid arthritis diagnosed according to ACR criteria and who had at least 8 tender and 6 swollen joints at baseline. In SC-II, 656 patients were randomized 2:1 to tocilizumab SC 162 mg every other week or placebo, in combination with non-biologic DMARD(s).
In study SC-II, inhibition of structural joint damage was assessed radiographically and expressed as a change from baseline in the van der Heijde modified mean total Sharp score (mTSS). At week 24, inhibition of structural damage was shown, with significantly less radiographic progression in patients receiving tocilizumab SC compared with placebo (mTSS of 0.62 vs. 1.23, p=0.0149 (van Elteren)). These results are consistent with those observed in patients treated with intravenous tocilizumab.
Quality of Life Outcomes – Intravenous Administration: Clinically significant improvements in disability index (HAQ-DI, Health Assessment Questionnaire Disability Index), fatigue (FACIT-Fatigue, Functional Assessment of Chronic Illness Therapy Fatigue) and improvement in both the physical (PCS, Physical Component Summary) and mental health (MCS, Mental Component Summary) domains of the SF-36 (Short Form 36) were observed in patients treated with 8 mg/kg tocilizumab (monotherapy or combination with DMARDs) compared to patients treated with MTX/DMARDs (Table 5).
At week 24, the proportion of 8 mg/kg tocilizumab treated patients showing a clinically relevant improvement in HAQ-DI (defined as an individual total score decrease of above 0.25), was significantly higher than among patients receiving placebo + MTX/DMARDs in all studies. During the open-label period of Study II the improvement in physical function has been maintained for up to 2 years. (See Table 5.)
Click on icon to see table/diagram/image
In study II, changes in PCS, MCS and FACIT-Fatigue at 52 weeks were 10.1
***, 5.4 and 8.4
**, respectively, in the TCZ 8 mg/kg + MTX group compared to 5.6, 3.8 and 5.5, respectively, in the Placebo plus MTX group. At Week 52, the mean change in HAQ-DI was -0.58 in the TCZ 8 mg/kg + MTX group compared with -0.39 in the placebo + MTX group. The mean change in HAQ-DI was maintained at Week 104 in the TCZ 8 mg/kg + MTX group (-0.61).
Quality of Life Outcomes – Subcutaneous Administration: In study SC-I, the mean decrease in HAQ-DI from baseline to week 24 was 0.6 for both tocilizumab SC 162 mg weekly and tocilizumab IV 8 mg/kg every 4 weeks. The proportion of patients achieving a clinically relevant improvement in HAQ-DI at week 24 (change from baseline of ≥ 0.3 units) was comparable in the tocilizumab SC every week group (65.2%) versus the tocilizumab IV 8 mg/kg group (67.4%), with a weighted difference in proportions of -2.3% (95% CI -8.1, 3.4). The SF-36 summary was split into mental and physical components. The mental component scores were similar between the groups, with a mean change from baseline at week 24 of 6.22 for the SC group and 6.54 for the IV group. The physical component scores were also similar between the groups, with mean change from baseline at week 24 of 9.49 for the SC group and 9.65 for the IV group.
Laboratory Evaluations: Treatment with 8 mg/kg tocilizumab in combination with DMARD/MTX or as monotherapy resulted in a highly statistically significant improvement in haemoglobin levels compared with placebo + MTX/DMARD (p<0.0001) at week 24. The greatest improvement was observed in patients with chronic anaemia associated with RA; mean haemoglobin levels increased by week 2 and remained within normal range through week 24.
A marked decrease in mean levels of acute phase reactants, CRP, ESR, and serum amyloid A occurred rapidly after tocilizumab administration. Consistent with the effect on acute phase reactants, treatment with tocilizumab was associated with reduction in platelet count within the normal range.
MTX naïve, Early RA: Study VI, a 2 year study with the planned primary analysis at week 52 evaluated 1162 MTX-naïve adult patients with moderate to severe, active early RA (mean disease duration ≤ 6 months). This study evaluated the efficacy of IV tocilizumab 4 or 8 mg/kg every 4 weeks/MTX combination therapy, IV tocilizumab 8 mg/kg monotherapy and MTX monotherapy in reducing the signs and symptoms and rate of progression of joint damage for 104 weeks. The primary endpoint was the proportion of patients achieving DAS28 remission (DAS28 below 2.6) at week 24. A significantly higher proportion of patients in the tocilizumab 8 mg/kg + MTX and tocilizumab monotherapy groups met the primary endpoint compared with MTX alone. The tocilizumab 8 mg/kg + MTX group also showed statistically significant results across the key secondary endpoints. Numerically greater responses compared with MTX alone were observed in the tocilizumab 8 mg/kg monotherapy group in all secondary endpoints, including radiographic endpoints. In this study, ACR/EULAR remission (Boolean and Index) were also analysed as pre-specified exploratory endpoints, with higher responses observed in the tocilizumab groups. The results from study VI are shown in Table 6. (See Table 6.)
Click on icon to see table/diagram/image
Monotherapy: tocilizumab versus adalimumab: Study WA19924 evaluated 326 patients with RA who were intolerant of MTX or where continued treatment with MTX was considered inappropriate (including MTX inadequate responders). Patients in the tocilizumab arm received an intravenous (IV) infusion of tocilizumab (8 mg/kg) every 4 weeks (q4w) and a subcutaneous (SC) placebo injection every 2 weeks (q2w). Patients in the adalimumab arm received an adalimumab SC injection (40 mg) q2w plus an IV placebo infusion q4w.
A statistically significant superior treatment effect was seen in favour of tocilizumab over adalimumab in control of disease activity from baseline to week 24 for the primary endpoint of change in DAS28 and for all secondary endpoints (Table 7). (See Table 7.)
Click on icon to see table/diagram/image
Cardiovascular Outcomes: Study WA25204 was a randomized, open-label (sponsor-blinded), 2-arm parallel-group, multi-center, non-inferiority, cardiovascular (CV) outcomes trial in patients with a diagnosis of moderate to severe RA. This CV safety study was designed to exclude a moderate increase in CV risk in patients treated with TCZ compared with a TNF inhibitor standard of care (etanercept [ETA]).
The study included 3,080 seropositive RA patients with active disease and an inadequate response to non-biologic disease-modifying anti-rheumatic drugs, who were aged ≥50 years with at least one additional CV risk factor beyond RA. Patients were randomized 1:1 to IV TCZ 8 mg/kg Q4W or SC ETA 50 mg QW and followed for an average of 3.2 years. The primary endpoint was the comparison of the time-to-first occurrence of any component of a composite of major adverse CV events (MACE; non-fatal myocardial infarction, non-fatal stroke, or CV death), with the final intent-to-treat analysis based on a total of 161 confirmed CV events reviewed by an independent and blinded adjudication committee.
Non-inferiority of TCZ to ETA for cardiovascular risk was determined by excluding a >80% relative increase in the risk of MACE. The primary endpoint was met such that a >43% increase in the risk of MACE could be excluded (hazard ratio [HR] comparing TCZ to ETA = 1.05; 95% CI = 0.77, 1.43).
Giant Cell Arteritis (GCA): Study WA28119 was a randomized, multi-center, double-blind placebo-controlled Phase III superiority study conducted to assess the efficacy and safety of tocilizumab in patients with GCA.
Two hundred and fifty one (251) patients with new-onset or relapsing GCA were enrolled and assigned to one of four treatment arms. The study consisted of a 52-week blinded period (Part 1), followed by a 104-week open-label extension (Part 2). The purpose of the Part 2 is to describe the long-term safety and maintenance of efficacy after 52 weeks of tocilizumab therapy, to explore the rate of relapse and the requirement for tocilizumab therapy beyond 52 weeks, and to gain insight into the potential long-term steroid-sparing effect of tocilizumab.
Two subcutaneous (SC) doses of tocilizumab (162 mg every week and 162 mg every other week) were compared to two different placebo control groups randomized 2:1:1:1.
All patients received background glucocorticoid (prednisone) therapy. Each of the tocilizumab-treated groups and one of the placebo-treated groups followed a pre-specified prednisone-taper regimen over 26 weeks, while the second placebo-treated group followed a pre-specified prednisone-taper regimen over 52 weeks designed to be more in keeping with standard practice.
The primary efficacy endpoint, assessed by the proportion of patients achieving steroid-free sustained remission at Week 52 on tocilizumab plus 26 weeks prednisone taper compared with placebo plus 26 weeks prednisone taper, was met (Table 8).
The key secondary efficacy endpoint, also based on the proportion of patients achieving sustained remission at Week 52, comparing tocilizumab plus 26 weeks prednisone taper with the longer placebo plus 52 weeks prednisone taper, was also met (Table 8).
A statistically significant superior treatment effect was seen in favour of tocilizumab over placebo in achieving steroid-free sustained remission at Week 52 on tocilizumab plus 26 weeks prednisone taper compared with placebo plus 26 weeks prednisone taper and with placebo plus 52 weeks prednisone taper.
The percentage of patients achieving sustained remission at week 52 are shown in Table 8 as follows.
Secondary Endpoints: The assessment of the time to first GCA flare showed a significantly lower risk of flare for the tocilizumab SC weekly group compared to placebo plus 26 weeks prednisone and placebo plus 52 weeks prednisone taper groups and for the tocilizumab SC every other weekly group compared to placebo plus 26 weeks prednisone (when compared at a 0.01 significance level). Tocilizumab SC weekly dose also showed a clinically meaningful decrease in the risk for flare compared to placebo plus 26 weeks prednisone in patients who entered the trial with relapsing GCA as well as those with new-onset disease (Table 8).
Cumulative glucocorticoid dose: The cumulative prednisone dose at Week 52 was significantly lower in the two tocilizumab dose groups compared to the two placebo groups (Table 8). In a separate analysis of the patients who received escape prednisone to treat GCA flare during the first 52 weeks, the cumulative prednisone dose varied greatly. The median doses for escape patients in the tocilizumab weekly and every other weekly groups were 3129.75 mg and 3847 mg, respectively – both considerably lower than in the placebo plus 26 weeks and the placebo plus 52 weeks prednisone taper groups, 4023.5 mg and 5389.5 mg respectively. (See Table 8.)
Click on icon to see table/diagram/image
Quality of Life Outcomes: In study WA28119, the SF-36 results were separated into the physical and mental component summary scores (PCS and MCS, respectively). The PCS mean change from baseline to week 52 was higher (showing more improvement) in the tocilizumab weekly and every other weekly dose groups [4.10, 2.76, respectively] than in the two placebo (PBO) groups [PBO plus 26 weeks; -0.28, PBO plus 52 weeks; -1.49], although only the comparison between tocilizumab weekly plus 26 weeks prednisone taper group and placebo plus 52 weeks prednisone taper group (5.59, 99% CI: 0.86, 10.32) showed a statistically significant difference (p=0.0024). For MCS, the mean change from baseline to week 52 for both tocilizumab weekly and every other weekly dose groups [7.28, 6.12, respectively] were higher than the placebo plus 52 weeks prednisone taper group [2.84] (although the differences were not statistically significant [p=0.0252 for weekly, p=0.1468 for every other weekly]) and similar to the placebo plus 26 weeks prednisone taper group [6.67].
The Patient's Global Assessment of disease activity was assessed on a 0-100mm Visual Analogue Scale (VAS). The mean change in Patient's global VAS from baseline at week 52 was lower (showing greater improvement) in the tocilizumab weekly and every other weekly dose groups [-19.0, -25.3, respectively] than in both placebo groups [PBO plus 26 weeks; -3.4, PBO plus 52 weeks; -7.2], although only the tocilizumab every other weekly plus 26 weeks prednisone taper group showed a statistically significance difference compared to placebo [PBO plus 26 weeks taper p=0.0059, and PBO plus 52 week taper p=0.0081].
FACIT-Fatigue change from baseline to Week 52 scores were calculated for all groups. The mean [SD] change scores were as follows: tocilizumab weekly plus 26 weeks 5.61 [10.115], tocilizumab every other weekly plus 26 weeks 1.81 [8.836], PBO plus 26 weeks 0.26 [10.702], and PBO plus 52 weeks -1.63 [6.753].
Change in EQ5D scores from baseline to week 52 were tocilizumab weekly plus 26 weeks 0.10 [0.198], tocilizumab every other weekly plus 26 weeks 0.05 [0.215], PBO plus 26 weeks 0.07 [0.293], and PBO plus 52 weeks -0.02 [0.159].
Higher scores signal improvement in both FACIT-Fatigue and EQ5D.
Polyarticular Juvenile Idiopathic Arthritis: The efficacy of intravenous tocilizumab was assessed in a three-part study including an open-label extension in children with active polyarticular juvenile idiopathic arthritis (pJIA). Part I consisted of a 16-week active tocilizumab treatment lead-in period (n=188) followed by Part II, a 24-week randomized double-blind placebo-controlled withdrawal period (ITT, n=163), followed by Part III, a 64-week open-label period. Eligible patients ≥ 30 kg received tocilizumab at 8 mg/kg for 4 doses. Patients below 30 kg were randomized 1:1 to receive either tocilizumab 8 mg/kg or 10 mg/kg IV every 4 weeks for 4 doses. Patients who completed Part I of the study and achieved at least a JIA ACR30 response at week 16 compared to baseline entered the blinded withdrawal period (Part II) of the study. In Part II, patients were randomized to tocilizumab (same dose received in Part I) or placebo in a 1:1 ratio was stratified by concurrent methotrexate use and concurrent corticosteroid use. Each patient continued in Part II of the study until Week 40 or until the patient satisfied JIA ACR30 flare criteria (relative to Week 16) and qualified for escape.
The primary endpoint was the proportion of patients with a JIA ACR30 flare at week 40 relative to week 16. Forty eight percent (48.1%, 39/81) of the patients treated with placebo flared compared with 25.6% (21/82) of TCZ-treated patients. These proportions were statistically significantly different (p=0.0024).
At the conclusion of Part I, JIA ACR 30/50/70/90 responses were 89.4%, 83.0%, 62.2%, and 26.1%, respectively.
During the withdrawal phase (Part II), the percent of patients achieving JIA ACR 30, 50, and 70 responses at Week 40 relative to baseline are shown in the table as follows. (See Table 9.)
Click on icon to see table/diagram/image
A 52-week, open-label, multi-center, PK-PD and safety study (WA28117) was conducted in paediatric patients with pJIA, aged 1 to 17 years old, to determine the appropriate subcutaneous dose of tocilizumab (TCZ) that achieved comparable PK/PD and safety profiles to the IV regimen.
Eligible patients received tocilizumab dosed according to body weight (BW), with patients weighing ≥30 kg (n = 25) dosed with 162 mg of tocilizumab every 2 weeks (Q2W) and patients weighing below 30 kg (n = 27) dosed with 162 mg of TCZ every 3 weeks (Q3W) for 52 weeks. Of these 52 patients, 37 (71%) were naive to tocilizumab and 15 (29%) had been receiving IV TCZ and switched to SC TCZ at baseline.
The SC TCZ regimens of 162 mg Q3W for patients weighing below 30 kg and of 162 mg Q2W for patients weighing ≥ 30 kg, respectively provided PK exposure and PD responses to support efficacy and safety outcomes similar to those achieved with the approved IV TCZ regimens for pJIA.
Exploratory efficacy results showed that SC tocilizumab improved median Juvenile Arthritis Disease Activity Score (JADAS)-71 for TCZ naïve patients and maintained the median JADAS-71 for patients who switched from IV to SC TCZ treatment over the entire course of the study for patients in both body weight groups (below 30 kg and ≥ 30 kg).
Systemic Juvenile Idiopathic Arthritis: The efficacy of intravenous tocilizumab for the treatment of active sJIA was assessed in a 12-week randomized, double blind, placebo-controlled, parallel group, 2-arm study. Patients (treated with or without MTX) were randomized (TCZ:placebo = 2:1) to one of two treatment groups, 75 patients received tocilizumab infusions every two weeks either 8 mg/kg for patients ≥30kg or 12 mg/kg for patients below 30 kg and 37 patients were assigned to receiving placebo infusions every two weeks. Corticosteroid tapering could occur from week six for patients who achieved a JIA ACR70 response. After 12 weeks or at the time of escape, due to disease worsening, patients were treated in the open-label extension phase at weight appropriate dosing.
The primary endpoint was the proportion of patients with at least 30% improvement in JIA ACR core set (JIA ACR30 response) at Week 12 and absence of fever (no temperature recording ≥ 37.5°C in the preceding 7 days). Eighty five percent (64/75) of the patients treated with TCZ and 24.3% (9/37) of placebo patients achieved this endpoint. These proportions were highly significantly different (p<0.0001).
The percent of patients achieving JIA ACR 30, 50, 70 and 90 responses are shown in the table as follows. Responses are maintained in the open label extension. (See Table 10.)
Click on icon to see table/diagram/image
Systemic Features: In those patients treated with tocilizumab, 85% who had fever due to sJIA at baseline were free of fever (no temperature recording ≥ 37.5°C in the preceding 14 days) at week 12 versus only 21% of placebo patients (p<0.0001) and 64% of tocilizumab treated patients with rash characteristic of sJIA at baseline were free of rash at week 12 versus 11% of placebo patients (p=0.0008).
There was a highly statistically significant reduction in pain for tocilizumab treated patients at week 12 in comparison to placebo patients. The adjusted mean change in the pain VAS after 12 weeks of tocilizumab treatment was a reduction of 41 points on a scale of 0-100 compared to a reduction of 1 for placebo patients (p<0.0001).
The responses for systemic features are maintained in the open label extension.
Corticosteroid Tapering: Of the 31 placebo and 70 tocilizumab patients receiving oral corticosteroids at baseline, 8 placebo and 48 tocilizumab patients achieved a JIA ACR70 response at week 6 or 8 enabling corticosteroid dose reduction. Seventeen (24%) tocilizumab patients versus 1 (3%) placebo patient were able to reduce the dose of corticosteroid by at least 20% without experiencing a subsequent JIA ACR30 flare or occurrence of systemic symptoms to week 12 (p=0.028). Reductions in corticosteroids continued, with 44 patients off oral corticosteroids, at week 44, while maintaining ACR responses.
Quality of Life: At week 12, the proportion of tocilizumab treated patients showing a minimally clinically important improvement in CHAQ-DI (defined as an individual total score decrease of ≥0.13) was significantly higher than in patients receiving placebo, 77% versus 19% (p<0.0001). Responses are maintained in the open label extension.
Laboratory Parameters: Fifty out of seventy five (67%) patients treated with tocilizumab had a haemoglobin below LLN at baseline. Forty (80%) of these patients with decreased haemoglobin had an increase in their haemoglobin to within the normal range at week 12, in comparison to only 2 out of 29 (7%) of placebo patients with haemoglobin below LLN at baseline (p<0.0001). Forty four (88%) tocilizumab patients with decreased haemoglobin at baseline had an increase in their haemoglobin by ≥10 g/L at week 6 versus 1 (3%) placebo patient (p<0.0001).
The proportion of tocilizumab treated patients with thrombocytosis at baseline who had a normal platelet count at week 12 was significantly higher than in the placebo patients, 90% versus 4%, (p<0.0001).
A marked decrease in mean levels of acute phase reactants, CRP, ESR, and serum amyloid A occurred rapidly after tocilizumab administration.
A Phase I, multi-centre, open-label, single arm study (NP25737) to evaluate the PK, safety and exploratory PD and efficacy of tocilizumab over 12 weeks in paediatric sJIA patients (N=11) under 2 years of age was conducted. Patients (treated with stable background therapy of corticosteroids, MTX, or non-steroidal anti-inflammatory drugs) received intravenous tocilizumab 12 mg/kg every two weeks. Patients who completed the 12-week period could continue to the optional extension period (a total of 52-weeks or until the age of 2 years, whichever was longer).
The primary PK endpoints (C
max, C
min and AUC
2weeks) of TCZ at steady-state in this study are within the ranges of these parameters observed in paediatric patients aged 2 to 17 years in Study WA18221.
The types of AEs observed during the 12-week evaluation period of Study NP25737 were consistent with the safety profile observed in the pivotal Phase III study (WA18221). Of the 11 patients aged under 2 years, three experienced serious hypersensitivity reactions, and three developed treatment induced anti-tocilizumab antibodies after the event. However, due to the small sample size, the low number of events and confounding factors, conclusions could not be drawn.
Exploratory efficacy results showed that tocilizumab improved the median JADAS-71 score over the course of the study for all patients. The observed PD responses in sIL6R, CRP, and ESR were also consistent with the pivotal Phase III study.
A 52-week, open-label, multi-centre, PK/PD and safety study (WA28118) was conducted in paediatric patients with sJIA, aged 1 to 17 years, to determine the appropriate SC dose of TCZ that achieved comparable PK/PD and safety profiles to the IV regimen.
Eligible patients received TCZ dosed according to body weight (BW), with patients weighing ≥ 30 kg (n = 26) dosed with 162 mg of TCZ every week (QW) and patients weighing below 30 kg (n = 25) dosed with 162 mg of TCZ every 10 days (Q10D; n=8) or every 2 weeks (Q2W; n=17) for 52 weeks. Of these 51 patients, 26 (51%) were naive to TCZ and 25 (49%) had been receiving IV TCZ and switched to SC TCZ at baseline.
Exploratory efficacy results showed that SC tocilizumab improved all exploratory efficacy parameters including Juvenile Arthritis Disease Activity Score (JADAS)-71, for TCZ naïve patients and maintained all exploratory efficacy parameters for patients who switched from IV to SC TCZ treatment over the entire course of the study for patients in both body weight groups (below 30 kg and ≥ 30 kg).
Pharmacokinetics: PK of tocilizumab is characterized by nonlinear elimination which is a combination of linear clearance and Michaelis-Menten elimination. The nonlinear part of tocilizumab elimination leads to an increase in exposure that is more than dose-proportional. The pharmacokinetic parameters of tocilizumab do not change with time. Due to the dependence of total clearance on tocilizumab serum concentrations, the half-life of tocilizumab is also concentration-dependent and varies depending on the serum concentration level. Population pharmacokinetic analyses in any patient population tested so far indicate no relationship between apparent clearance and the presence of anti-drug antibodies.
Rheumatoid Arthritis: The pharmacokinetics in healthy subjects and RA patients suggest that PK is similar between the two populations.
The table as follows shows model predicted secondary PK parameters at each of the four approved dose regimens. The population PK (popPK) model was developed from an analysis dataset composed of an IV dataset of 1793 patients from studies WA17822, WA17824, WA18062 and WA18063 and IV and SC dataset of 1759 patients from studies WA22762 and NA25220. C
mean is included in the table since for dosing regimens with different inter-dose interval, the mean concentration over the dosing period characterizes the comparative exposure better than AUC
T. (See Table 11.)
Click on icon to see table/diagram/image
At high serum concentrations, when total clearance of tocilizumab is dominated by linear clearance, a terminal half-life of approximately 21.5 days was derived from the population parameter estimates.
While after IV administration maximum concentration (C
max) increased dose-proportionally between doses of 4 and 8 mg/kg IV every 4 weeks, a greater than dose-proportional increase was observed in the average concentration (C
mean) and trough concentration (C
trough). At steady-state, C
mean and C
trough were 3.2 and 32 fold higher at 8 mg/kg as compared to 4 mg/kg, respectively. Exposures after the 162 mg SC QW regimen were greater by 4.6 (C
mean) to 7.5 fold (C
trough) compared to the 162 SC Q2W regimen.
The accumulation ratios for AUC and C
max after multiple doses of 4 and 8 mg/kg Q4W are low, while the accumulation ratios are higher for C
trough (2.62 and 2.47). Accumulation ratios after multiple doses of either SC regimen were higher than after IV regimen with the highest ratios for C
trough (6.02 and 6.30). The higher accumulation for C
trough was expected based on the nonlinear clearance contribution at lower concentrations.
For C
max, more than 90% of the steady-state was reached after the 1
st IV infusion, and after the 12
th SC and the 5
th SC injection in QW and Q2W regimens respectively. For AUC
T and C
mean, 90% of the steady-state was reached after the 1
st and 3
rd infusion for the 4 mg/kg and 8 mg/kg IV, respectively, and after the 6
th and 12
th injections for the 162 mg SC Q2W and QW regimens respectively. For C
trough, approximately 90% of the steady-state was reached after the 4
th IV infusion, the 6
th and 12
th injections for the respective SC regimens.
Population PK analysis identified body weight as a significant covariate impacting pharmacokinetics of tocilizumab. When given IV on a mg/kg basis, individuals with body weight ≥ 100 kg are predicted to have mean steady-state exposures higher than mean values for the patient population. Therefore, tocilizumab doses exceeding 800 mg per infusion are not recommended in patients ≥ 100 kg (see Dosage & Administration). Due to the flat dosing employed for SC administration of tocilizumab, no modifications are necessary by this dosing route.
Giant Cell Arteritis (GCA): The pharmacokinetics of tocilizumab in GCA patients were determined using a popPK model from an analysis dataset composed of 149 GCA patients treated with 162 mg SC every week or with 162 mg SC every other week. The developed model had the same structure as the population PK model developed earlier based on data from RA patients. (See Table 12.)
Click on icon to see table/diagram/image
The steady-state profile following the tocilizumab weekly dose was almost flat, with very little fluctuations between trough and peak values, while there were substantial fluctuations for the tocilizumab every other week dose. Approximately 90% of the steady-state (AUC
T) was reached by Week 14 in the every other weekly and Week 17 in the weekly dose groups.
Polyarticular Juvenile Idiopathic Arthritis: The pharmacokinetics of tocilizumab in pJIA patients was characterized by a population pharmacokinetic analysis which included 237 patients who were treated with 8 mg/kg IV every 4 weeks (patients weighing ≥ 30 kg), 10 mg/kg IV every 4 weeks (patients weighing below 30 kg), 162 mg SC every 2 weeks (patients weighing ≥ 30 kg), or 162 mg SC every 3 weeks (patients weighing below 30 kg). (See Table 13.)
Click on icon to see table/diagram/image
After IV dosing, approximately 90% of the steady-state was reached by Week 12 for the 10 mg/kg (BW < 30 kg), and by Week 16 for the 8 mg/kg (BW ≥ 30 kg) dose. After SC dosing, approximately 90% of the steady-state was reached by Week 12 for both the 162 mg SC Q2W and Q3W regimens.
Systemic Juvenile Idiopathic Arthritis: The pharmacokinetics of tocilizumab in sJIA patients was characterized by a population pharmacokinetic analysis which included 140 patients who were treated with 8 mg/kg IV every 2 weeks (patients weighing ≥ 30 kg), 12 mg/kg IV every 2 weeks (patients weighing below 30 kg), 162 mg SC every week (patients weighing ≥ 30 kg), 162 mg SC every 10 days or every 2 weeks (patients weighing below 30 kg). (See Table 14.)
Click on icon to see table/diagram/image
After IV dosing, approximately 90% of the steady-state was reached by Week 8 for both the 12 mg/kg and 8 mg/kg Q2W regimens. After SC dosing, approximately 90% of the steady-state was reached by Week 12 for both the 162 mg QW and Q2W regimens.
The pharmacokinetics of tocilizumab were similar in paediatric patients under 2 years compared to patients over 2 years of age with a body weight below 30 kg from a regimen of 12 mg/kg IV tocilizumab given every 2 weeks.
Absorption: Following SC dosing in RA and GCA patients, the absorption half-life was around 4 days. The bioavailability for the SC formulation was 80%.
In GCA patients, the median values of T
max were 3 days after the tocilizumab weekly dose and 4.5 days after the tocilizumab every other week dose.
Following SC dosing in pJIA patients, the absorption half-life was around 2 days, and the bioavailability for the SC formulation in pJIA patients was 96%.
Following SC dosing in sJIA patients, the absorption half-life was around 2 days, and the bioavailability for the SC formulation in sJIA patients was 95%.
Distribution: Following IV dosing, tocilizumab undergoes biphasic elimination from the circulation. In rheumatoid arthritis patients the central volume of distribution was 3.5 L, the peripheral volume of distribution was 2.9 L resulting in a volume of distribution at steady state of 6.4 L.
In GCA patients, the central volume of distribution was 4.09 L, the peripheral volume of distribution was 3.37 L resulting in a volume of distribution at steady state of 7.46 L.
In paediatric patients with pJIA, the central volume of distribution was 1.98 L, the peripheral volume of distribution was 2.1 L, resulting in a volume of distribution at steady state of 4.08 L.
In paediatric patients with sJIA, the central volume of distribution was 1.87 L, the peripheral volume of distribution was 2.14 L resulting in a volume of distribution at steady state of 4.01 L.
Metabolism: No text.
Elimination: The total clearance of tocilizumab was concentration-dependent and is the sum of the linear clearance and the nonlinear clearance. The linear clearance was estimated as a parameter in the population pharmacokinetic analysis and was 12.5 mL/h in RA patients, 6.7 mL/h in GCA patients, 5.8 mL/h in paediatric patients with polyarticular juvenile idiopathic arthritis and 5.7 mL/h in paediatric patients with systemic juvenile idiopathic arthritis. The concentration-dependent nonlinear clearance plays a major role at low tocilizumab concentrations. Once the nonlinear clearance pathway is saturated, at higher tocilizumab concentrations, clearance is mainly determined by the linear clearance. Due to dependence of total clearance on tocilizumab serum concentrations, t
½ of tocilizumab is also concentration-dependent and can only be calculated at a given serum concentration level.
In RA patients, for intravenous administration, the concentration-dependent apparent t
½ is up to 11 days for 4 mg/kg and 13 days for 8 mg/kg every 4 weeks in patients with RA at steady-state. For subcutaneous administration, the concentration-dependent apparent t
½ is up to 13 days for 162 mg every week and 5 days for 162 mg every other week in patients with RA at steady-state. At high serum concentrations, when total clearance of tocilizumab is dominated by linear clearance, a terminal t
½ of approximately 21.5 days was derived from the population parameter estimates.
In GCA patients, at steady state, the effective t
½ of tocilizumab varied between 18.3 and 18.9 days for 162 mg weekly regimen, and between 4.2 and 7.9 days for 162 mg every other weekly regimen. At high serum concentrations, when total clearance of tocilizumab is dominated by linear clearance, an effective t
½ of approximately 32 days was derived from the population parameter estimates.
In children with pJIA, the effective t
½ of IV tocilizumab is up to 17 days for the two body weight categories (8 mg/kg for body weight ≥ 30 kg or 10 mg/kg for body weight below 30 kg) during a dosing interval at steady state. After subcutaneous administration, the effective t
½ of tocilizumab in pJIA patients is up to 10 days for the two body weight categories (Q2W regimen for body weight ≥30 kg or Q3W regimen for body weight below 30 kg) during a dosing interval at steady state.
In children with sJIA, the effective t
½ of IV tocilizumab is up to 16 days for both the 12 mg/kg and 8 mg/kg Q2W regimens during a dosing interval at steady-state. Following subcutaneous administration, the effective t
½ of tocilizumab in sJIA patients is up to 14 days for both the 162 mg QW and Q2W regimens during a dosing interval at steady state.
Pharmacokinetics in Special Populations: Hepatic Impairment: No formal study of the effect of hepatic impairment on the pharmacokinetics of tocilizumab was conducted.
Renal Impairment: No formal study of the effect of renal impairment on the pharmacokinetics of tocilizumab was conducted.
Most of the patients in the RA and GCA studies population pharmacokinetic analysis had normal renal function or mild renal impairment. Mild renal impairment (estimated creatinine clearance based on Cockcroft-Gault formula) did not impact the pharmacokinetics of tocilizumab.
Approximately one-third of the patients in the study WA28119 had moderate renal impairment at baseline (estimated creatinine clearance of 30-59 mL/min). No impact on tocilizumab exposure was noted in these patients.
No dose adjustment is required in patients with mild or moderate renal impairment.
Other special populations: Population pharmacokinetic analyses in adult RA and GCA patients showed that age, sex and race did not affect pharmacokinetics of tocilizumab. No dose adjustment is necessary for these demographic factors.
Toxicology: Nonclinical Safety: Carcinogenicity: A carcinogenicity study of tocilizumab has not been conducted. Available preclinical data, showed the contribution of the pleiotropic cytokine IL-6 to malignant progression and apoptosis resistance of various cancer types. These data do not suggest a relevant risk for cancer initiation and progression under therapy with tocilizumab. Accordingly, proliferate lesions have not been observed in a chronic cynomolgus monkey 6-month toxicity study nor were they described in IL-6 knock-out mice under chronic IL-6 depletion.
Genotoxicity: Standard genotoxicity studies with tocilizumab in both prokaryotic and eukaryotic cells were all negative.
Impairment of Fertility: Nonclinical data do not suggest an effect on fertility under treatment with an analogue of tocilizumab. Effects on endocrine active organs or on organs of the reproductive system were not seen in a chronic cynomolgus monkey toxicity study, nor was the reproductive performance affected in IL-6 deficient male and female mice.
Reproductive Toxicity: When tocilizumab was administered intravenously to cynomolgus monkeys during early gestation, no direct or indirect harmful effects on pregnancy or embryo-foetal development were observed.
Other: In an embryo-foetal toxicity study conducted in cynomolgus monkeys a slight increase of abortion/embryo-foetal death was observed with high systemic cumulative exposure (above 100 times human exposure) in the 50 mg/kg/day high-dose group compared to placebo and other low-dose groups. The abortion incidence was within the historical background for the cynomolgus monkey in captivity and the individual cases of abortions/embryo-foetal death did not show any consistent relationship to dosing or duration of dosing with tocilizumab. Although IL-6 does not seem to be a critical cytokine for either foetal growth or the immunological control of the maternal/foetal interface, a relation of this finding to tocilizumab cannot be excluded.
Transfer of a murine analogue of tocilizumab into the milk of lactating mice has been observed.
Treatment with a murine analogue did not exert toxicity in juvenile mice. In particular, there was no impairment of skeletal growth, immune function and sexual maturation.
The non-clinical safety profile of tocilizumab in the cynomolgus monkey does not suggest a difference between IV and SC routes of administration.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image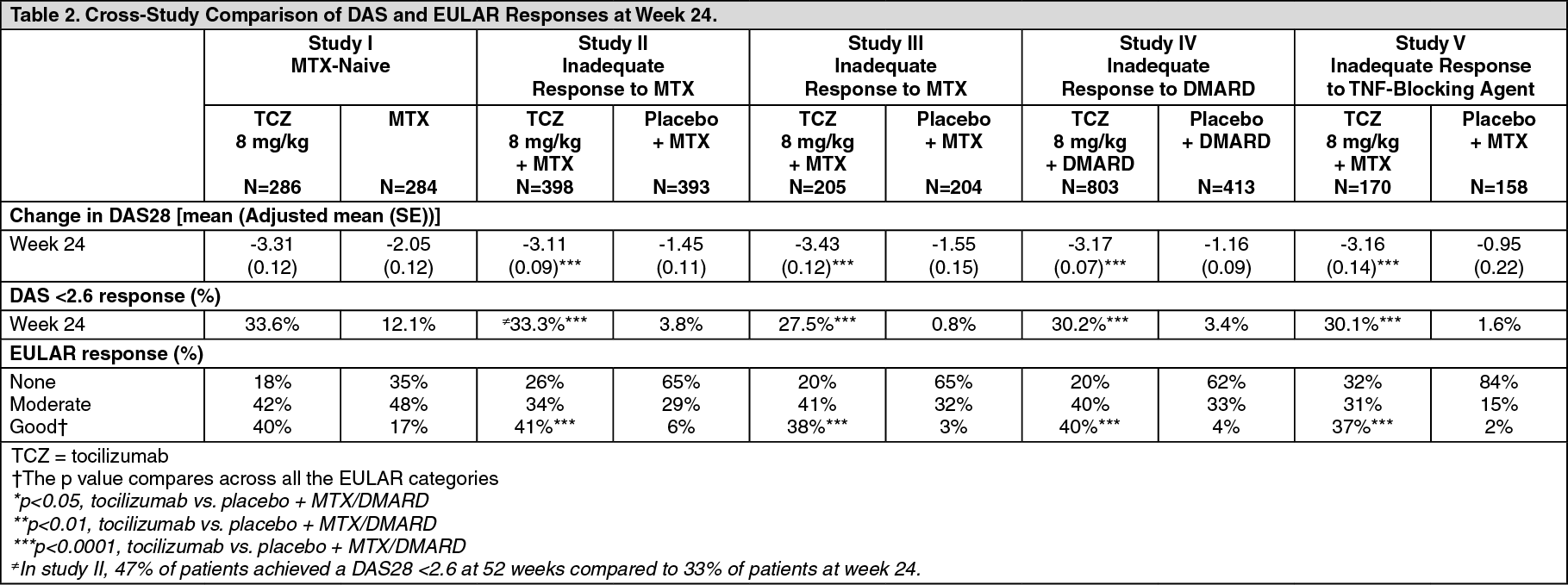 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image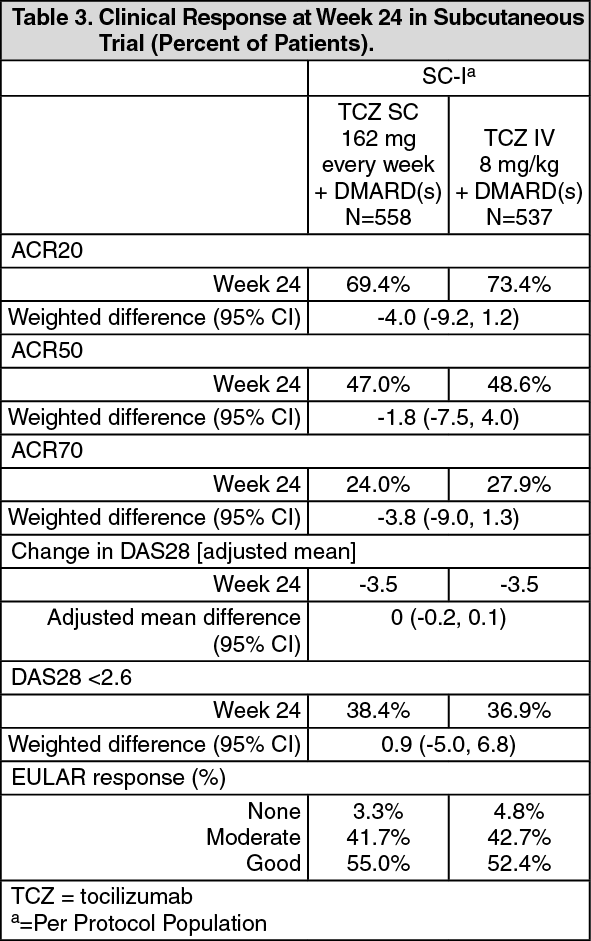 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image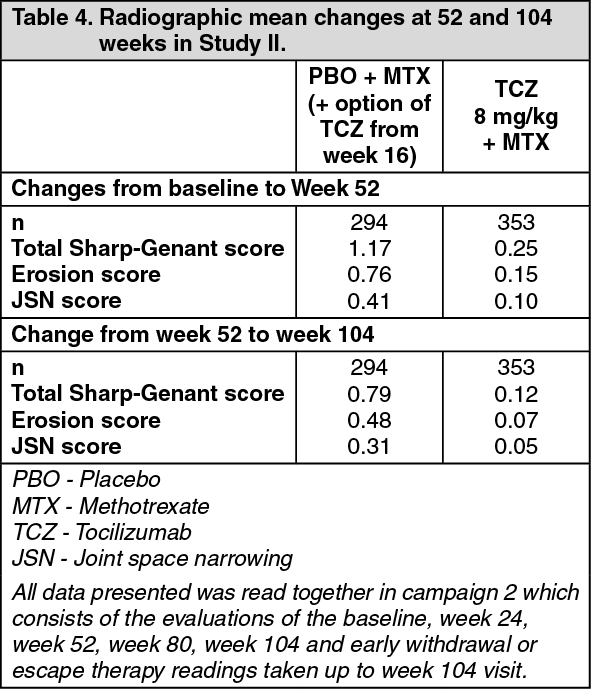 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image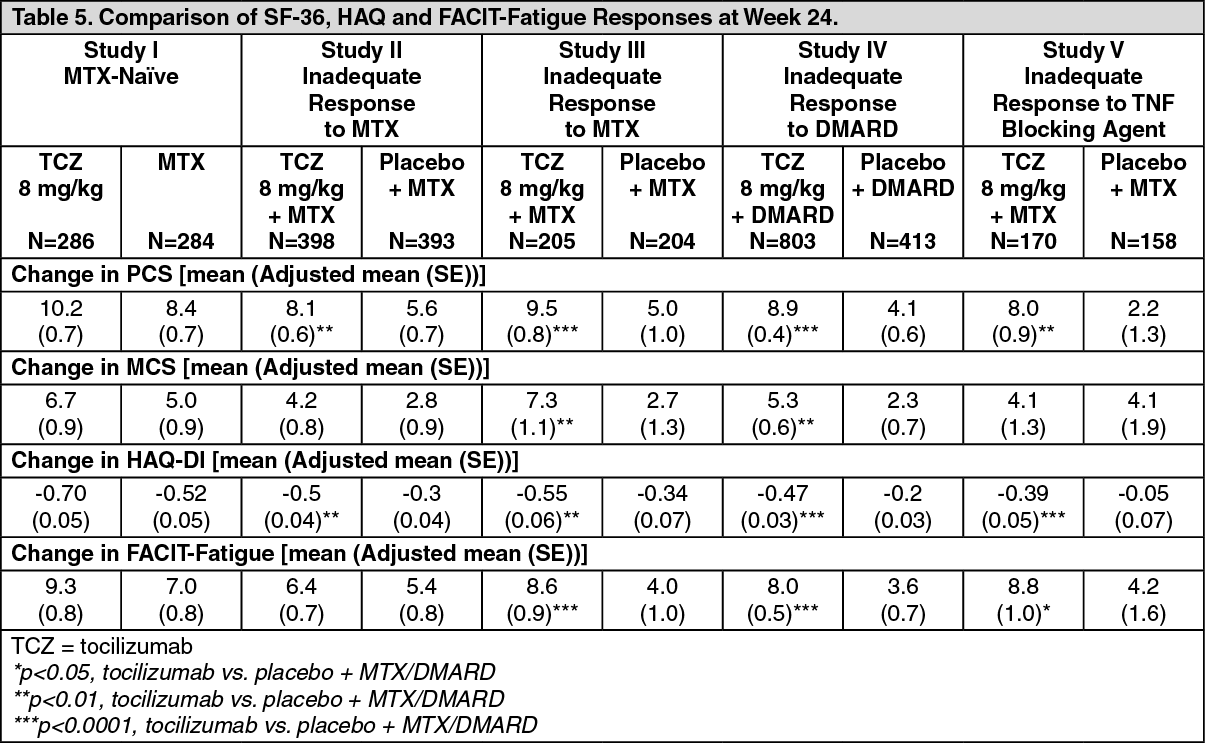 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image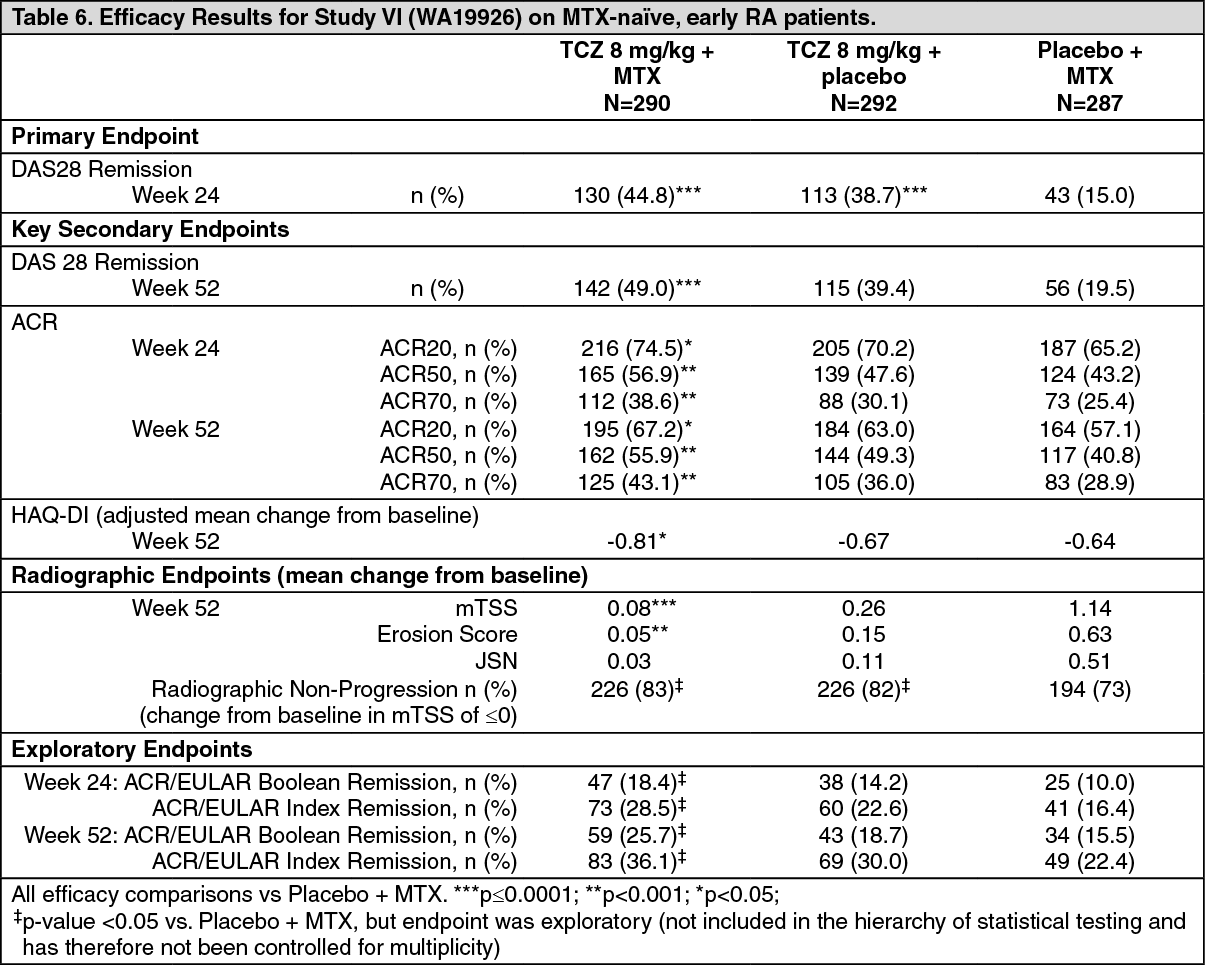 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image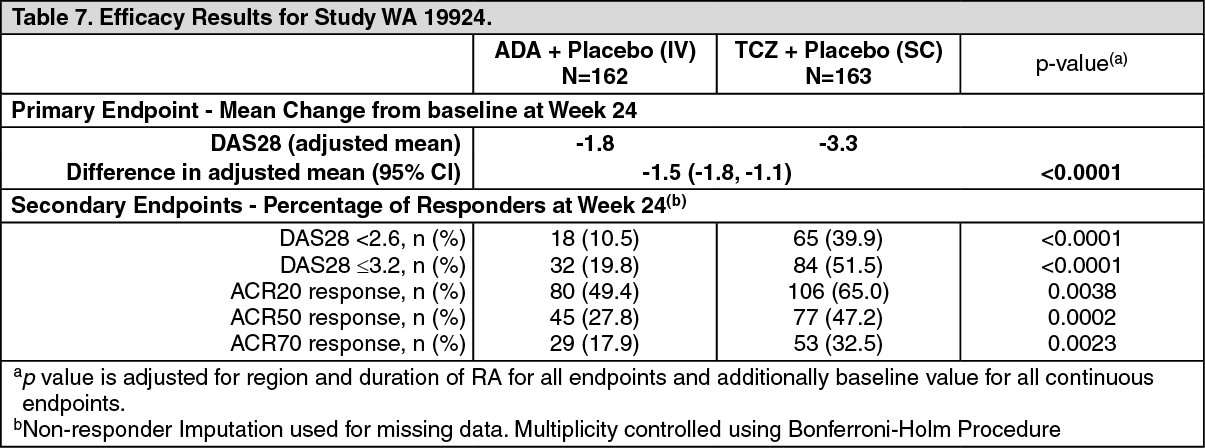 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image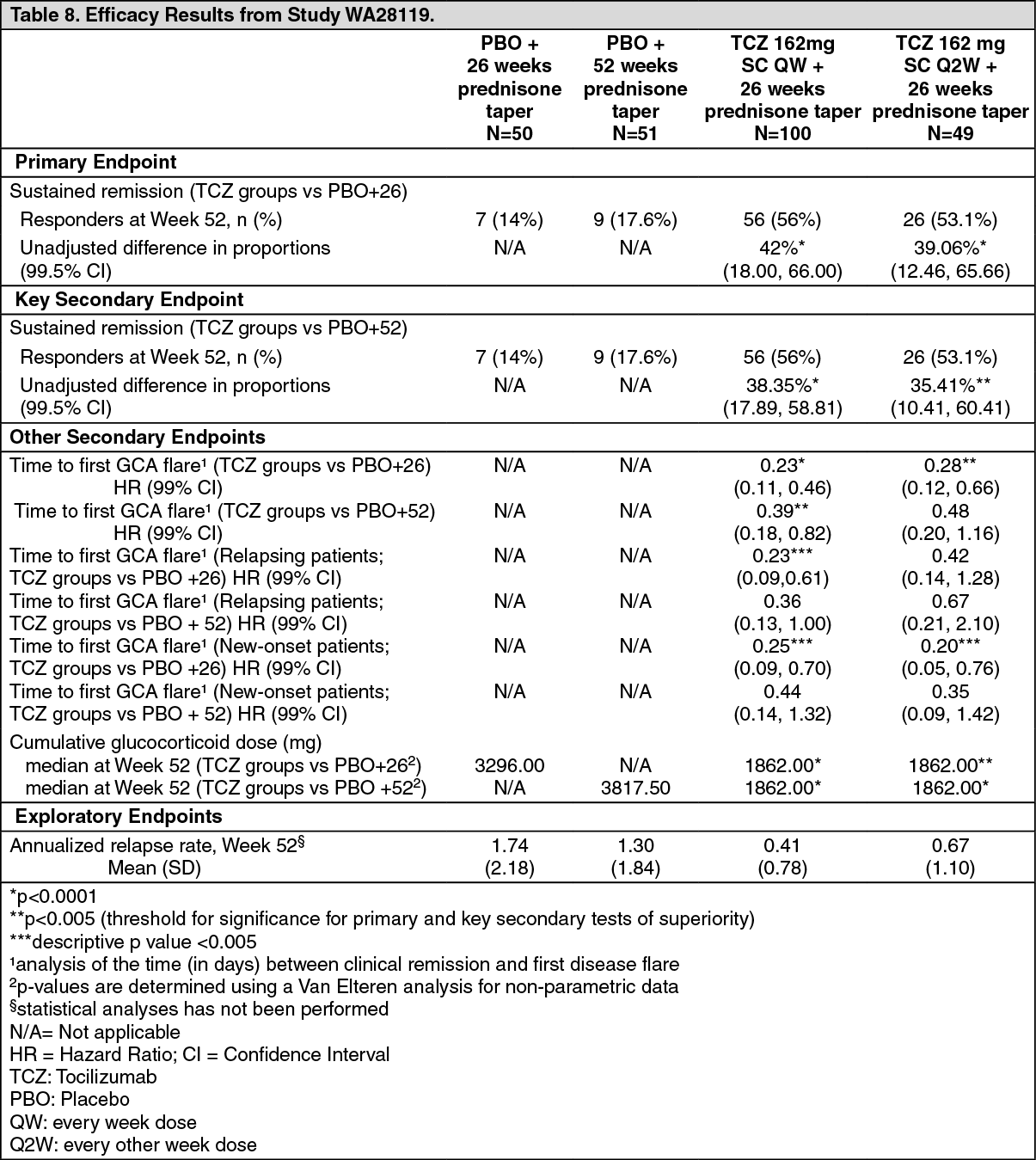 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image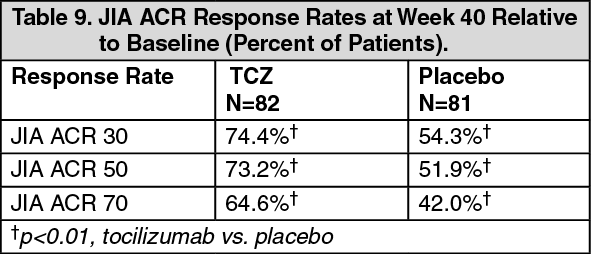 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image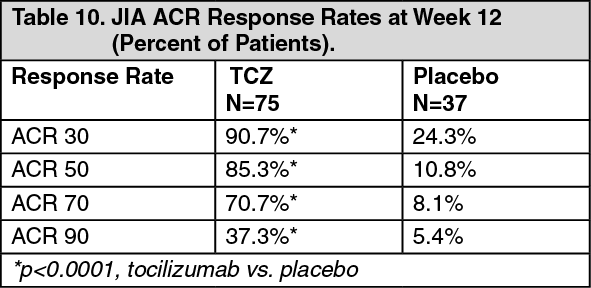 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image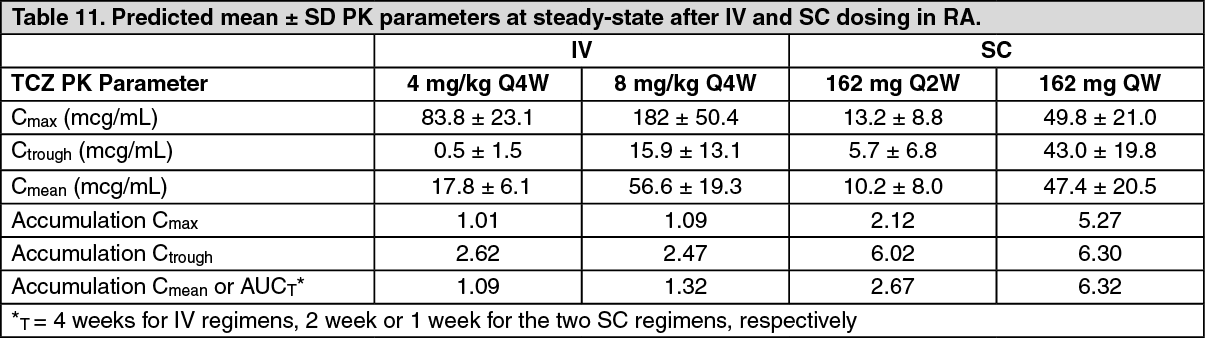 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image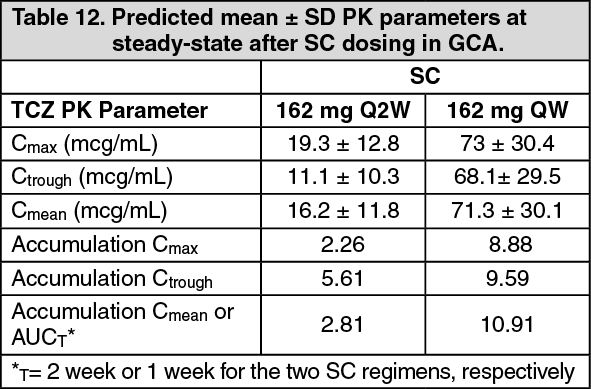 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image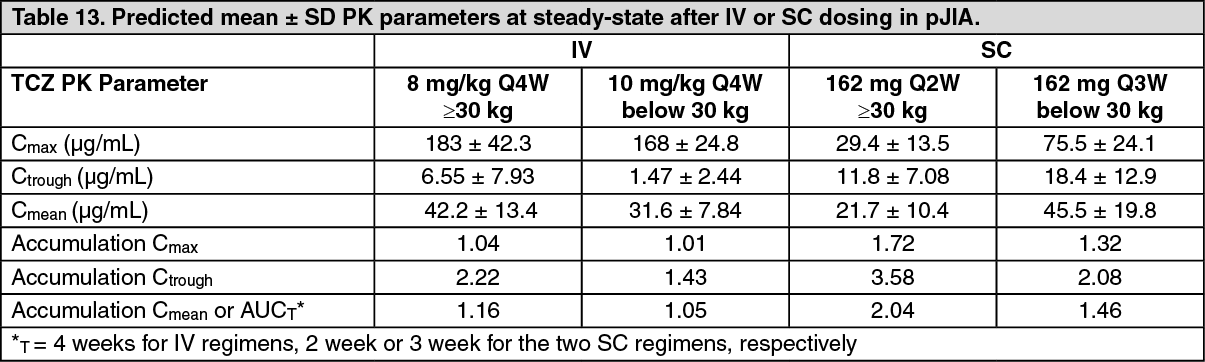 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image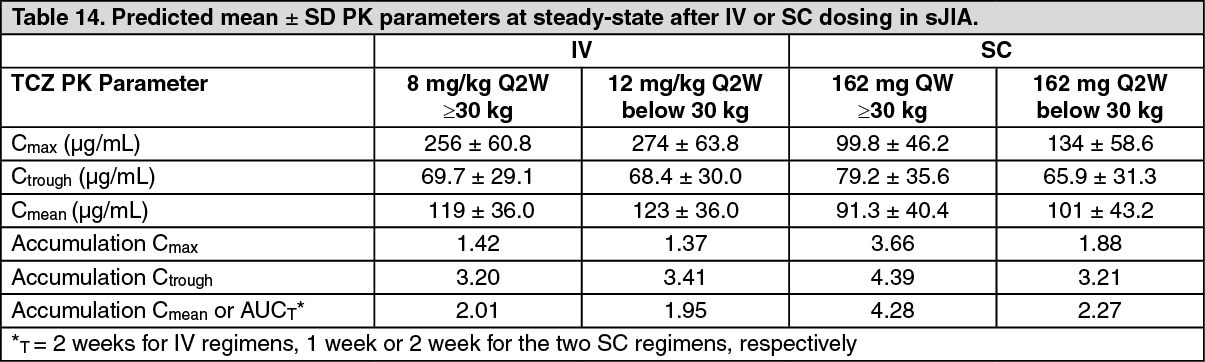 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
